Below are **10 high-yield, exam-level, detailed case scenarios on Abortion**, each followed by **complete clinical reasoning + management** (clear, guideline-based, 2025).
No images included as requested.
---
# **🔶 CASE SCENARIO 1 — Threatened Abortion**
### **Case**
A 7-week pregnant woman presents with light vaginal bleeding and mild lower abdominal discomfort. No tissue passed. Cervical os is closed. Ultrasound shows a live intrauterine pregnancy with cardiac activity. Hemodynamics stable. She is Rh-negative.
### **Management**
* **Expectant management** (no need for hospital admission).
* **Avoid strenuous activity**; pelvic rest.
* **Progesterone (if indicated):**
* Dydrogesterone 10 mg BID *or* micronized progesterone 200 mg vaginal nightly (especially in recurrent miscarriage).
* **Anti-D** 50–100 µg since she is Rh-negative.
* **Return immediately** if bleeding increases or pain worsens.
* **Repeat ultrasound in 1 week**.
---
# **🔶 CASE SCENARIO 2 — Inevitable Abortion**
### **Case**
A 10-week pregnant woman comes with heavy bleeding and cramping. The cervical os is **open** and products of conception are visible.
### **Management**
* **Stabilize:** IV fluids, vitals monitoring.
* **Evacuation options:**
* **Medical:** Misoprostol 600–800 µg vaginal/SL.
* **Surgical:** **Manual Vacuum Aspiration (MVA)** or suction curettage (preferred if heavy bleeding).
* **Analgesics + antibiotics prophylaxis:**
* Doxycycline 100 mg BID × 5 days.
* **Anti-D** if Rh-negative.
* **Follow-up ultrasound** in 7–14 days.
---
# **🔶 CASE SCENARIO 3 — Incomplete Abortion**
### **Case**
A 9-week pregnancy with history of passage of some tissue. Ongoing bleeding, os slightly open. USG shows retained products.
A 6-week pregnancy with previous bleeding and passage of tissue. Now asymptomatic. USG shows empty uterus.
### **Management**
* **No intervention needed.**
* **Analgesics PRN.**
* **Anti-D** if Rh-negative.
* **Discuss contraception** options.
* **Advise on warning signs** (fever, heavy bleeding).
---
# **🔶 CASE SCENARIO 5 — Missed Abortion**
### **Case**
A 12-week pregnant woman with no fetal heartbeat on USG. Cervical os is closed. No bleeding. Diagnosis: **missed abortion**.
### **Management**
Options:
### **1. Medical** (preferred up to 12–14 weeks)
* **Mifepristone 200 mg orally**, followed 24 hours later by
**Misoprostol 800 µg vaginal/SL**
* Repeat misoprostol 400 µg after 3 hours if incomplete.
### **2. Surgical**
* **Suction evacuation** (recommended if patient desires quick procedure).
### **Supportive**
* **Anti-D** if Rh-negative.
* **Analgesics**.
* **Follow-up USG** after 1–2 weeks.
---
# **🔶 CASE SCENARIO 6 — Septic Abortion (Emergency)**
### **Case**
A woman with 8-week pregnancy underwent an unsafe abortion. Now has fever (39°C), foul-smelling discharge, tachycardia, abdominal guarding, BP 90/60.
### **Management — LIFE-SAVING**
### **1. Stabilize**
* IV fluids, O2, monitoring.
* Blood cultures, CBC, CRP, lactate.
* Start antibiotics immediately (do not wait for labs):
### **2. Antibiotics**
* **Clindamycin 900 mg IV q8h + Gentamicin 5–7 mg/kg/day**
* Add **Metronidazole 500 mg IV q8h** if anaerobic risk high.
### **3. Evacuation**
* **Uterine evacuation after stabilization** (MVA/ suction).
* **Suction evacuation** if retained tissue present.
* **Tranexamic acid 1 g IV** if heavy bleeding.
* **Uterotonics:**
* Misoprostol 800 µg rectal
* Oxytocin infusion
* **Blood transfusion** as needed.
* **Anti-D** if Rh-negative.
---
# ✅ Want more?
I can also provide:
✔ **15–30 MCQs based on these cases**
✔ **HTML–CSS–JS exam-mode quiz**
✔ **Flowcharts for abortion management**
✔ **Long-form blog article (SEO optimized)**
Just tell me what you want next.
Below is the **complete, exam-ready, exhaustive medical reference on ABORTION** (MTP/ miscarriage/ induced abortion), written *only in text* as you asked. No images included.
---
# **ABORTION — COMPLETE DETAILED MEDICAL NOTES (2025)**
*(Definition → Pathophysiology → Causes → Classification → Clinical features → Investigations → Differential Diagnoses → Management → Complications → Drugs with full details)*
---
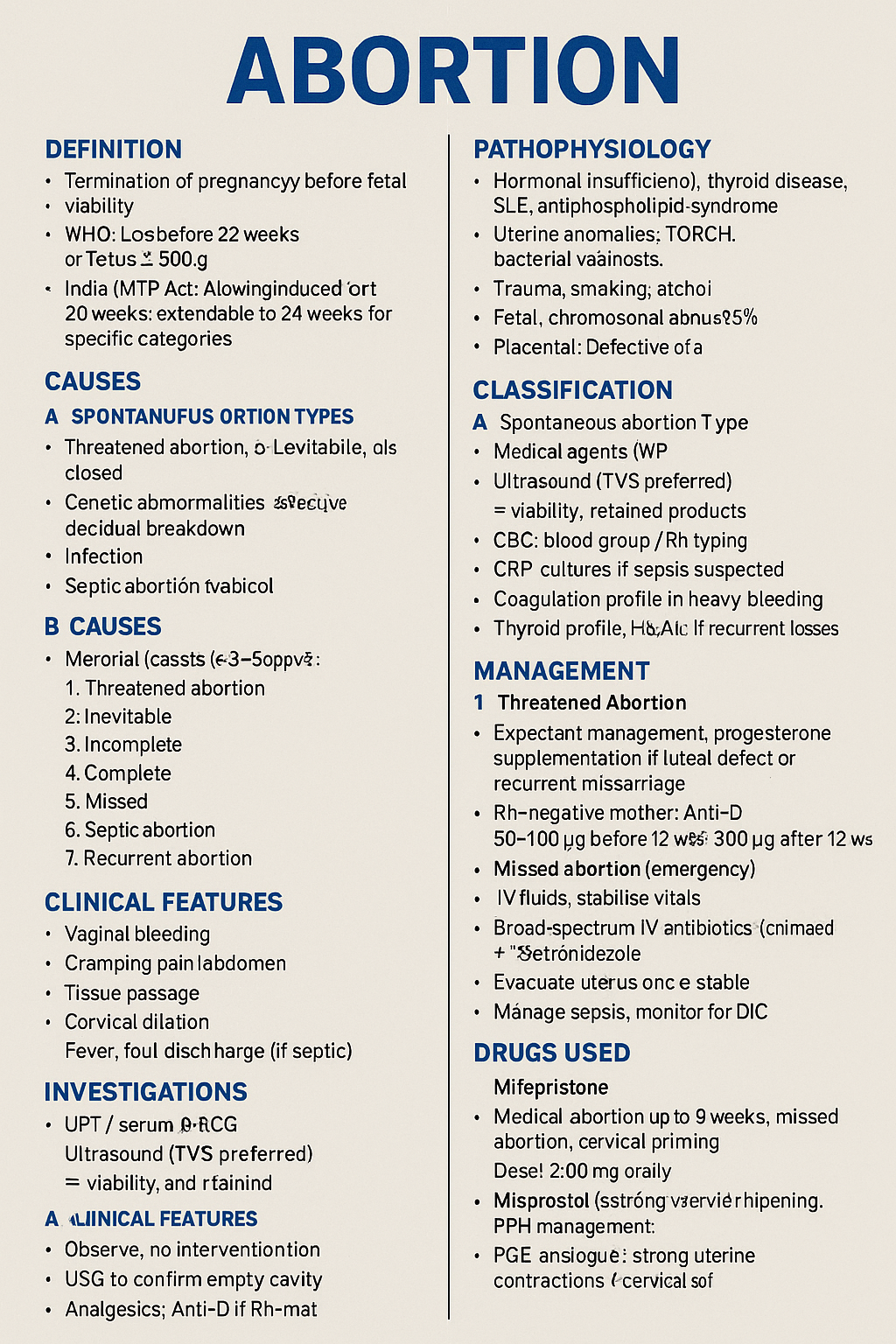
## **1. DEFINITION**
Abortion = **termination of pregnancy before fetal viability**.
* **WHO**: Loss before **22 weeks** or fetus < **500 g**.
* **India (MTP Act)**: Induced abortion allowed up to **20 weeks** (with conditions); extended to **24 weeks** for special categories.
* Misoprostol induction regimen
* D&E by trained provider
---
## **C. Complete Abortion**
* Observe, no intervention
* USG to confirm empty cavity
* Analgesics; Anti-D if Rh– mother
---
## **D. Missed Abortion**
* **Medical**: Mifepristone 200 mg PO then misoprostol 800 µg after 24 hrs
* **Surgical**: MVA/ suction evacuation
* Anti-D if Rh–
---
## **E. Septic Abortion (Emergency)**
* IV fluids, stabilize vitals
* **Broad-spectrum IV antibiotics** (example: clindamycin + gentamicin ± metronidazole)
* Evacuate uterus once stable
* Manage sepsis, monitor for shock and DIC
---
## **F. Induced Abortion (MTP Act India)**
### **Medical Abortion (up to 9 weeks recommended)**
1. **Mifepristone 200 mg orally**
2. Followed 24–48 hrs by
**Misoprostol 800 µg** vaginal/sub-lingual/buccal
3. Repeat 400 µg after 3 hrs if needed
4. Follow-up USG at 1–2 weeks
* Abortion: 800 µg vaginal/SL/buccal; repeat 400 µg if required.
**Pharmacokinetics:** Rapid absorption; hepatic metabolism.
**Side Effects:** Pain, diarrhea, fever, chills.
**Serious:** Uterine rupture (rare in scarred uterus).
**Contraindications:** Suspected ectopic pregnancy.
**Interactions:** None major.
**Monitoring:** Pain, bleeding.
**Counselling:** Cramping is expected; hydrate; seek help if bleeding heavy.
---
## **3. ANTIBIOTICS (SEPTIC ABORTION)**
### **Clindamycin + Gentamicin ± Metronidazole**
**Indication:** Severe pelvic infection.
**Mechanism:**
* Clindamycin → inhibits 50S ribosome
* Gentamicin → inhibits 30S ribosome
* Metronidazole → DNA damage in anaerobes
**Dosing:**
* Clindamycin 900 mg IV q8h
* Gentamicin 5–7 mg/kg IV daily
* Metronidazole 500 mg IV q8h
**Side Effects:** Nephrotoxicity, ototoxicity (gentamicin).
**Monitoring:** Renal function, vitals, WBC.
---
# **11. COUNSELLING POINTS**
* Expect bleeding for 1–2 weeks after medical abortion
* No intercourse for 1–2 weeks
* Contraception planning after abortion
* Warning signs: heavy bleeding, fever, foul discharge, severe pain
* Rhesus negative mothers need **Anti-D**
---
# **12. FOLLOW-UP**
* USG after 7–14 days to ensure complete evacuation
* Rule out anemia, infection
* Psychological support if needed
---
If you want, I can also provide:
✅ A **short exam-revision summary**,
✅ **MCQs**,
✅ **Flowcharts**,
✅ **Case-based questions**,
—all **in text only**, without images.
Just tell me **“Give MCQs”** or **“Give flowcharts”**.