* Mother records movements daily.
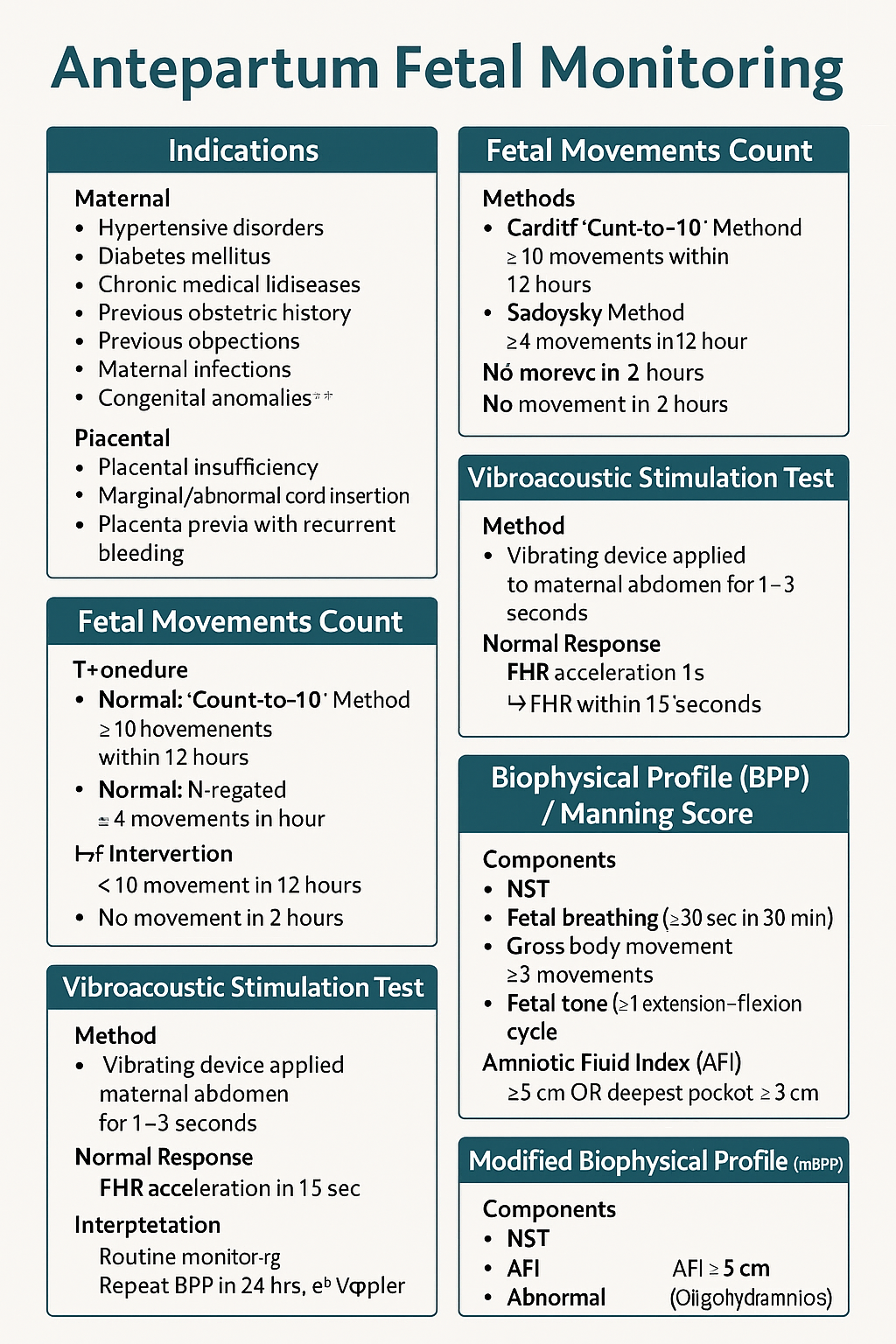
* **Normal:** 10 movements within 12 hours.
### **B. Sadovsky Method**
* Count movements for 1 hour after meals.
* **Normal:** ≥4 movements/hour.
### **When to worry?**
* **<10 movements in 12 hours**
* **<4 movements in 1 hour**
* **No movement in 2 hours** → urgent evaluation (NST/BPP)
### **Management of Decreased Fetal Movements**
1. Immediate **NST**
2. If NST non-reactive → **BPP**
3. If BPP equivocal → **Doppler studies**
4. If evidence of fetal compromise → **Delivery based on GA**
---
# **3️⃣ Non-Stress Test (NST)**
NST measures **fetal heart rate accelerations** in response to fetal movements via cardiotocography.
### **Procedure**
* Done after **28–32 weeks** (mature autonomic nervous system).
* Duration: **20 minutes** (extend to 40 minutes if needed).
---
## **Interpretation (Reactive vs Non-Reactive)**
### ✔ **Reactive NST (Normal)**
* **≥2 accelerations** in 20 minutes
* Acceleration criteria:
* **≥15 bpm for ≥15 sec** (≥32 weeks)
* **≥10 bpm for ≥10 sec** (<32 weeks)
### **AFI is chronic marker**; NST is acute marker.
---
# ⭐ **HIGH-YIELD VALUES (MUST REVISE)**
* Reactive NST: **≥2 accelerations** (15 × 15)
* Tone: 1 flexion–extension
* Breathing: ≥1 episode ≥30 sec
* Movement: ≥3 body movements
* AFI: Normal ≥5 cm
* Modified BPP = NST + AFI
* Sleep cycle: **20–40 min** → extend NST to 40 min
---
If you'd like, I can also generate:
✅ **Hard MCQs with explanations (HTML + CSS + JS exam mode)**
✅ **SEO-optimized title + meta description**
✅ **Case scenarios**
✅ **Infographic/diagram image**
Just tell me **what you want next.**
Below are **25 high-yield, clinically realistic, exam-oriented case scenarios** on **Antepartum Fetal Monitoring**, each with **stepwise management** exactly as required for NEET PG / INI-CET level.
---
# ⭐ **25 CASE SCENARIOS WITH DETAILED MANAGEMENT**
# **1️⃣ Case Scenario – Decreased Fetal Movements at 34 Weeks**
A 28-year-old G2P1 at 34 weeks reports **no fetal movements for 8 hours**.
### **Management**
1. Immediate **NST**
2. If **reactive** → reassure, daily kick count
3. If **non-reactive** → extend to 40 min
4. If still non-reactive → **VAST**
5. If remains non-reactive → **BPP**
6. * **BPP ≥8** → Follow-up
* **BPP ≤4** → Deliver based on GA
---
# **2️⃣ Case Scenario – Non-Reactive NST in a Diabetic Mother**
GDM on insulin at 36 weeks undergoes NST → **non-reactive** after 40 minutes.
### **Management**
1. Perform **VAST**
2. If reactive → repeat NST in 1 week
3. If still non-reactive → **Full BPP**
4. If BPP score **≤4** → Plan delivery
5. Assess **AFI & Doppler** for placental insufficiency
---
# **3️⃣ Case Scenario – Oligohydramnios with IUGR**
30-year-old at 32 weeks with **AFI = 4 cm**, EFW <10th percentile.
### **Management**
1. Start **modified BPP (NST + AFI)**
2. Daily NST
3. Doppler: **Umbilical artery S/D ratio**
4. If AEDF/REDF → **Immediate delivery**
5. If NST non-reactive → full BPP
6. Steroids if <34 weeks
---
# **4️⃣ Case – Post-Dated Pregnancy (41 Weeks)**
Patient at 41+2 weeks shows decreased fetal movement.
### **Management**
1. **NST + AFI**
2. If NST reactive & AFI normal → induce labour within 24–48 hrs
3. If NST non-reactive → BPP
4. BPP ≤6 → Deliver
5. Continuous intrapartum monitoring
---
# **5️⃣ Case – Preeclampsia with Severe Features**
32 weeks, BP 160/110, proteinuria +++, fetus active.
### **Management**
1. Daily **NST**
2. Twice-weekly **BPP**
3. Doppler (UA + MCA) weekly
4. Magnesium sulfate for seizure prophylaxis
5. Deliver at 34 weeks or earlier if fetal compromise
---
# **6️⃣ Case – Chronic Hypertension with Reduced Movements**
35-year-old with chronic HTN reports <4 kicks in 1 hr.
### **Management**
1. Immediate **NST**
2. If non-reactive → BPP
3. If AFI <5 → suspect placental insufficiency
4. Admit, daily surveillance
5. Deliver if BPP ≤4 or Doppler abnormal
---
# **7️⃣ Case – IUGR with Normal NST**
29 weeks, IUGR but **reactive NST**.
### **Management**
1. Continue **twice-weekly NST**
2. Weekly Doppler (UA/ MCA/ CPR ratio)
3. Growth scan every 2 weeks
4. Deliver if Doppler deteriorates or NST becomes abnormal
---
# **8️⃣ Case – Polyhydramnios with GDM**
30-year-old with polyhydramnios, NST reactive.
### **Management**
1. Twice-weekly NST
2. AFI monitoring
3. Doppler weekly
4. Induce at 38–39 weeks
5. Prepare for shoulder dystocia risk
---
# **9️⃣ Case – Decreased Fetal Movement in Obese Mother**
NST shows **baseline variability minimal**.
### **Management**
1. Rule out maternal meds, sleep cycle
2. Extend NST + VAST
3. If still abnormal → BPP
4. Deliver if BPP ≤4
1. Continue monitoring
2. Do not interpret variability during MgSO₄ therapy
3. Use **BPP** instead of NST
---
# **1️⃣9️⃣ Case – Poorly Controlled Diabetes**
36 weeks, polyhydramnios + macrosomia.
### **Management**
1. NST every 2–3 days
2. Weekly BPP
3. Deliver at 38 weeks
4. Prepare for shoulder dystocia
---
# **2️⃣0️⃣ Case – Maternal Dehydration**
NST non-reactive.
### **Management**
1. Give IV fluids
2. Repeat NST
3. If reactive → dehydration cause
4. If persists → BPP
---
# **2️⃣1️⃣ Case – Postpartum Hemorrhage Risk Mother**
Placenta previa major.
### **Management**
1. Weekly NST
2. BPP if NST abnormal
3. Plan elective C-section at 36–37 weeks
---
# **2️⃣2️⃣ Case – Fetal Tachycardia**
FHR 170 bpm in NST.
### **Management**
1. Exclude maternal fever, dehydration, drugs
2. Treat maternal cause
3. If persists → BPP + Doppler
4. Consider delivery if fetal compromise
---
# **2️⃣3️⃣ Case – Mother on Sedatives**
NST non-reactive.
### **Management**
1. Document medication effect
2. Perform BPP instead of repeating NST
3. Reassure if BPP normal
---
# **2️⃣4️⃣ Case – Sudden IUD Suspicion**
No FHR detected in NST.
### **Management**
1. Confirm with ultrasound
2. Evaluate cause (abruption, cord accident)
3. Manage according to GA and maternal stability
---
# **2️⃣5️⃣ Case – Preterm (<32 Weeks) Non-Reactive NST**
At 30 weeks, NST non-reactive.
### **Management**
1. Extend NST to 40 min
2. Apply VAST
3. If still non-reactive → BPP
4. If BPP ≤4 → Deliver after steroid cover
5. If BPP normal → prematurity likely cause
---
# ⭐ If you want, I can also provide:
✅ **25 Hard MCQs (HTML + CSS + JS exam mode)**
✅ **Infographic image**
✅ **Full HTML post with SEO + JSON-LD schema**