Below are **30 detailed intrapartum fetal monitoring case scenarios with complete management**, written in **NEET PG / INI-CET exam style**.
Each scenario includes **clinical context → CTG finding → diagnosis → step-wise management**.
---
# ✅ **30 CASE SCENARIOS WITH DETAILED MANAGEMENT (Intrapartum Fetal Monitoring)**
---
## **1️⃣ Case — Late Decelerations in a Preeclamptic Mother**
A 25-year-old primigravida, 4 cm dilated, on oxytocin. CTG shows **recurrent late decelerations**, baseline 150, variability <5 bpm.
### **Diagnosis**
Uteroplacental insufficiency from **preeclampsia + hyperstimulation**.
### **Management**
1. Stop oxytocin
2. Left lateral position
3. IV fluids
4. If contraction frequency >5/10 min → **tocolysis (terbutaline 0.25 mg SC)**
5. If no improvement → **FBS**
6. If pH <7.20 or tracing deteriorates → **Emergency LSCS**
---
## **2️⃣ Case — Variable Decelerations with Oligohydramnios**
G2P1, term labor, CTG shows **variable decelerations with shoulders**, adequate variability.
### **Diagnosis**
Cord compression due to oligohydramnios.
### **Management**
1. Maternal repositioning
2. Amnioinfusion
3. Continue labor if variability normal
4. If severe recurrent variables + loss of variability → expedite delivery
## **2️⃣6️⃣ Case — Placental Abruption Suspected**
Pain + bleeding + fetal tachycardia → later bradycardia.
### **Management**
1. Stabilize mother
2. Immediate LSCS if fetus alive
3. Vaginal delivery only if imminent
---
## **2️⃣7️⃣ Case — IUGR Baby with Recurrent Late Decelerations**
CTG: late decels + reduced variability.
### **Management**
1. Intrauterine resuscitation
2. No role for prolonged labor
3. **Expedite delivery**
---
## **2️⃣8️⃣ Case — Maternal Seizure (Eclampsia)**
CTG: prolonged decel.
### **Management**
1. Stabilize mother (MgSO₄, airway)
2. Left lateral position
3. If fetal recovery absent → LSCS
---
## **2️⃣9️⃣ Case — Vaginal Birth After Multiple Variables**
CTG mostly reassuring except mild variables.
### **Management**
1. Continue monitoring
2. Check for cord issues
3. No intervention unless severe
---
## **3️⃣0️⃣ Case — Failure of Fetal Response to Scalp Stimulation**
Minimal variability, no acceleration after stimulation.
### **Diagnosis**
Hypoxia suspected.
### **Management**
1. FBS if available
2. If pH abnormal → immediate delivery
3. If not available → treat as pathological CTG → expedite delivery
---
If you want, I can also produce:
✅ **HTML + CSS + JS EXAM MODE MCQs (25/30/50)**
✅ **SEO title/description/keywords**
✅ **A medical diagram image for intrapartum fetal monitoring**
Just say **“generate MCQs”**, **“generate image”**, or **“give SEO”**.
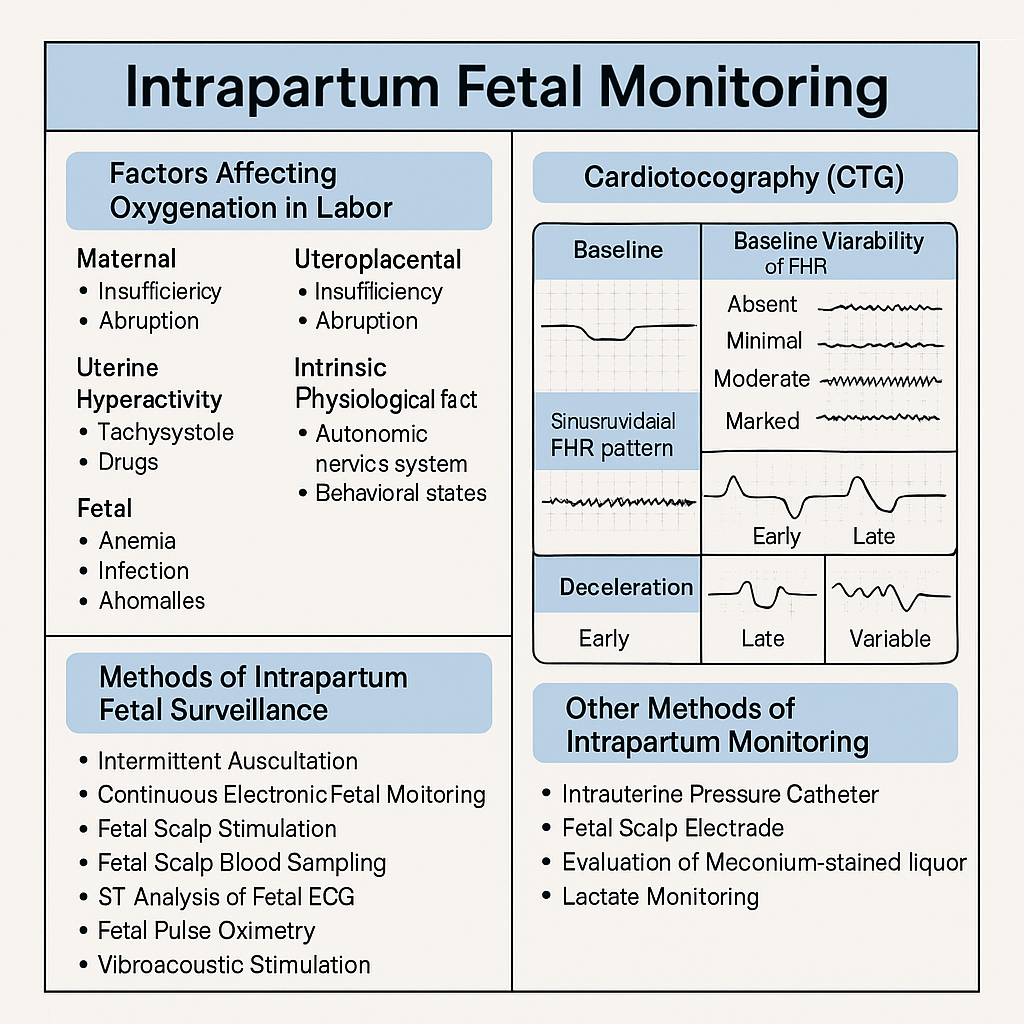
Below is your **complete, concise-but-exhaustive master reference** on **Intrapartum Fetal Monitoring** — fully aligned with NEET PG / INI-CET high-yield requirements.
* Mirror contractions.
* Due to **head compression**.
* **Benign, no treatment.**
### **B. Late Decelerations**
* Begin after the contraction peak → return after contraction ends.
* Due to **uteroplacental insufficiency**.
* **Always concerning**, esp. with absent variability.
### **C. Variable Decelerations**
* Abrupt fall in FHR, variable shape.
* Due to **cord compression**.
* May have "shoulders" (pre- & post-acceleration).
* Severe if >60 bpm drop lasting >60 sec.
### **D. Prolonged Deceleration**
* FHR drop ≥15 bpm lasting **2–10 min**.
* > 10 min = change in baseline.
### **E. Sinusoidal Pattern (MOST IMPORTANT)**
**True Sinusoidal Pattern**
* Smooth, regular, sine-wave oscillation (3–5 cycles/min)
* Amplitude 5–15 bpm
* No variability, no accelerations
* **Causes:**
* Severe fetal anemia (Rh isoimmunization, fetomaternal hemorrhage)
* Twin-to-twin transfusion
* Hypoxia late stage
* **Immediate delivery required**
**Pseudo-sinusoidal:**
* Seen with opioids — benign.
---
## **4️⃣ NICE 2024 Categories of CTG Interpretation**
| Topic | Key Points |
| ------------------------------- | ------------------------------- |
| Best indicator of fetal hypoxia | **Reduced variability** |
| Worst CTG sign | **Sinusoidal pattern** |
| Earliest sign of hypoxia | **Tachycardia** |
| Most common deceleration | **Variable (cord compression)** |
---
If you want, I can also generate:
✅ SEO title, description & keywords
✅ 25 hard case-based MCQs (HTML + CSS + JS EXAM MODE)
✅ 25 case scenarios with management
✅ Medical diagram image (via image generator)