Below is a **complete, concise-but-exhaustive medical reference** for **Rh-negative pregnancy**, followed by **SEO title, description, keywords**, and an **auto-generated image**.
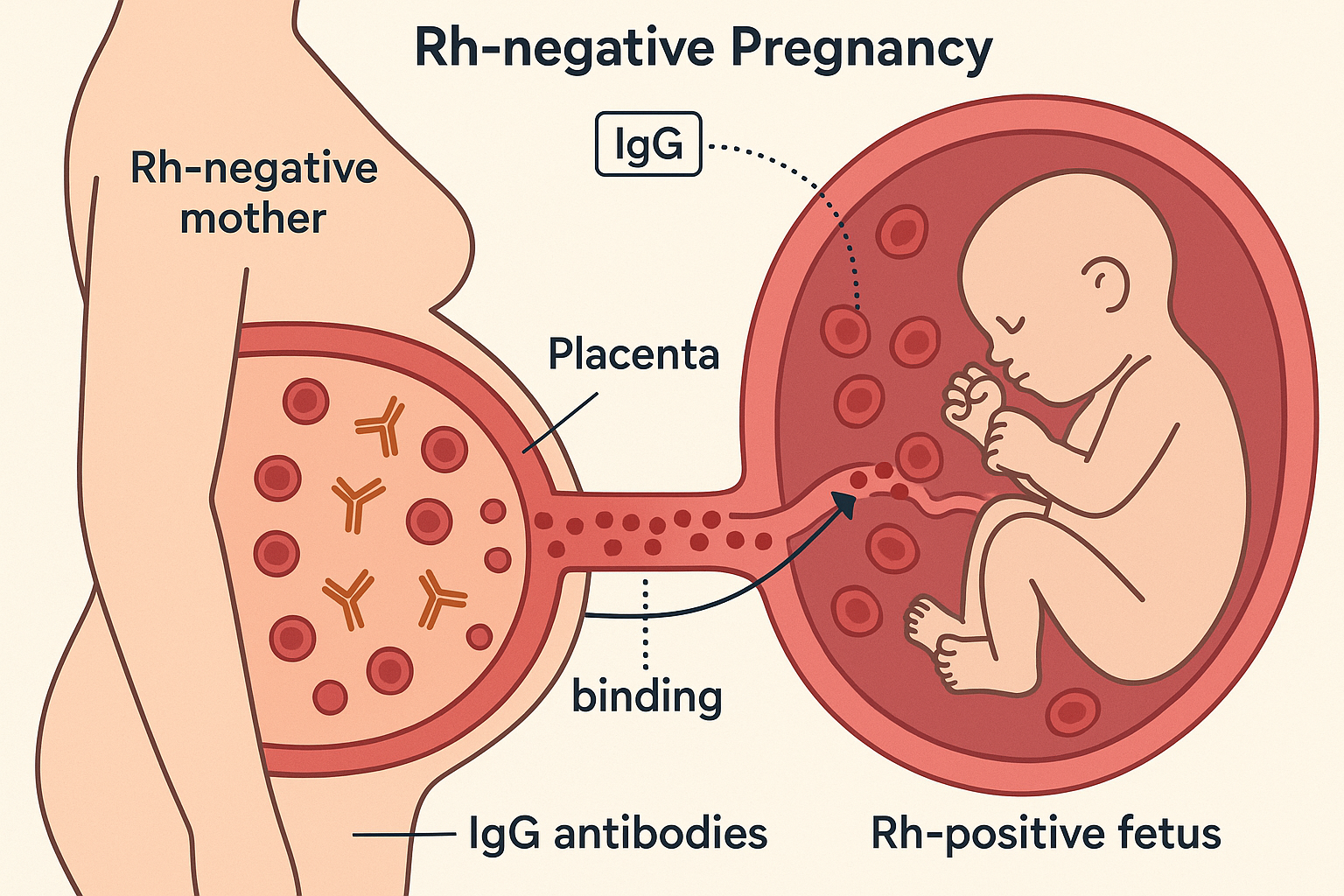
**Rh-negative pregnancy** occurs when a pregnant woman is **Rh-negative (D antigen absent)** and her fetus is **Rh-positive (inherited from father)** → risk of **Rh alloimmunization** and **Hemolytic Disease of Fetus & Newborn (HDFN)** if fetal RBCs enter maternal circulation.
Used to calculate fetal bleed volume → adjust Anti-D dose.
---
## **B. ALREADY SENSITIZED (ICT POSITIVE)**
Goal → **Monitor & treat fetal anemia**
### **Steps**
1. Determine **fetal RhD status** (cffDNA or amniocentesis).
2. If RhD positive → monitor **antibody titres** up to 28 weeks, then every 2 weeks.
3. Once titre ≥1:16 → perform **MCA-PSV Doppler** weekly.
4. If MCA-PSV >1.5 MoM → **severe fetal anemia** → manage:
---
### **Management of Severe Fetal Anemia**
* **Intrauterine transfusion (IUT)** via cordocentesis
* O negative, leukocyte-reduced, irradiated RBCs
* Repeat every 2–4 weeks until 34 weeks
* Delivery planned at **37–38 weeks** after last IUT
* If hydrops persists → consider **early delivery** (≥32 weeks) if lung maturity adequate
---
# 7️⃣ **Newborn Management**
* **Direct Coombs Test**
* Check hemoglobin, bilirubin, reticulocyte count
* **Phototherapy**
* **Exchange transfusion** if severe hyperbilirubinemia
* IVIG may reduce need for exchange transfusion
---
# 8️⃣ **Complications**
### **Maternal**
* Alloimmunization (permanent)
### **Fetal**
* Hemolytic disease
* Hydrops fetalis
* Intrauterine death
* Prematurity due to early delivery
* Neurodevelopmental impairment (kernicterus)
A complete, exam-ready guide to Rh-negative pregnancy: pathophysiology, causes, investigations, anti-D prophylaxis, management of sensitized vs unsensitized mothers, fetal monitoring, and complications.