Teratogenic Exposure in Pregnancy: 25 High-Yield Case Scenarios, Diagnosis & Management | Complete 2025 Obstetrics Guide
Below is a **compact but fully comprehensive, exam-ready medical note** on **Teratogenic Exposure in Pregnancy**, covering radiation, drugs, infections, maternal diseases, hyperthermia, SLE, PKU, mechanisms, critical periods, dose effects, and hallmark malformations.
✅ **Hard NEET PG/INICET MCQs (20 or 50)**
✅ **HTML exam-mode MCQ file**
✅ **Concise PDF note**
✅ **Infographic image**
Just tell me what format you want next.
Here are **25 high-yield, exam-level case scenarios with detailed diagnosis + management**, fully aligned with **NEET PG / INICET clinical reasoning**.
# ⭐ **25 DETAILED CASE SCENARIOS WITH MANAGEMENT**
---
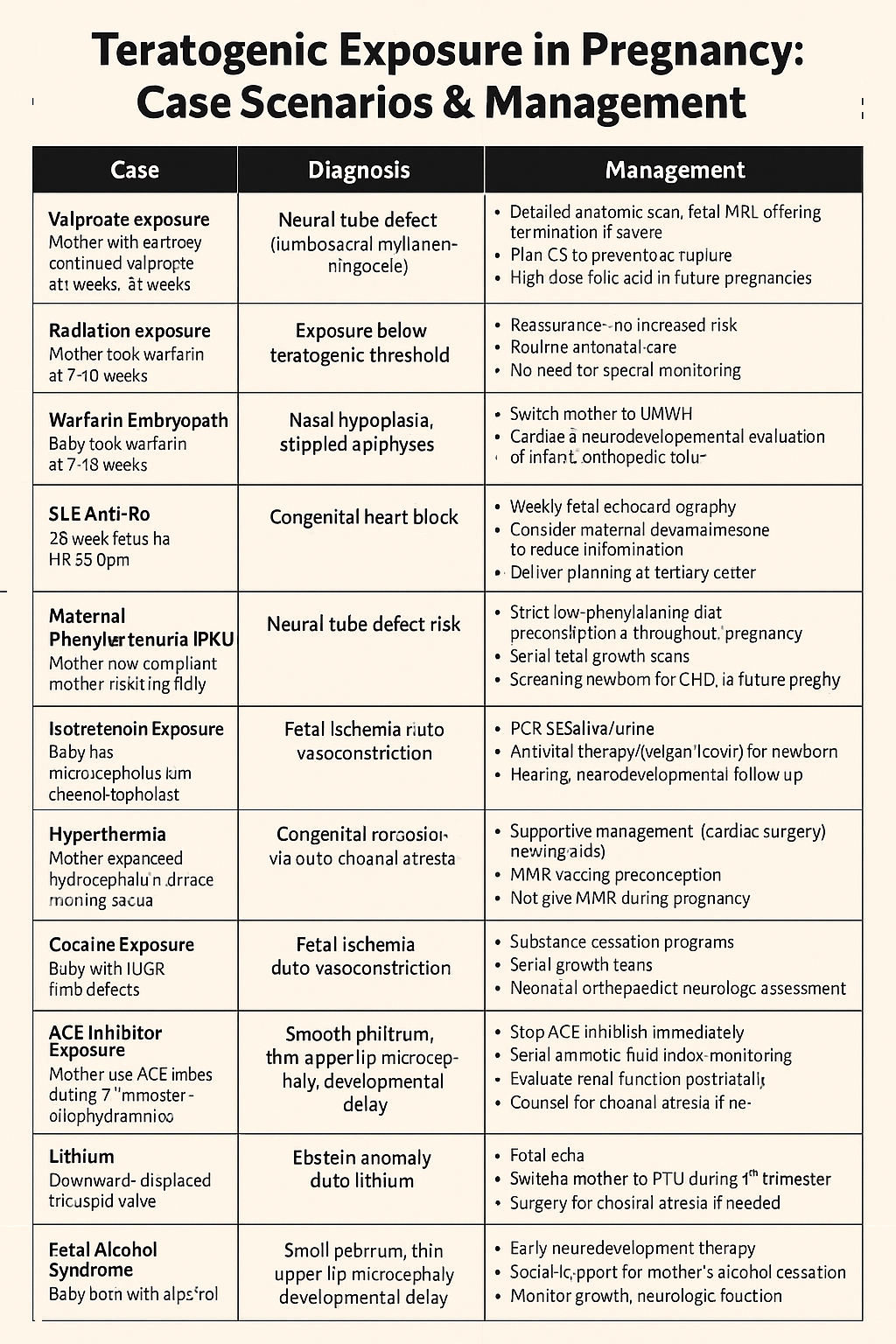
# **1. Valproate Exposure → Neural Tube Defect**
**Case:**
A 24-year-old pregnant woman with epilepsy continued valproate during early pregnancy. At 18 weeks, USG reveals **lumbosacral myelomeningocele**.
* Detailed anatomic scan + fetal MRI
* Offer termination if severe
* If continuing pregnancy → plan for CS to prevent sac rupture
* High-dose folic acid in future pregnancies (4 mg/day)
---
# **2. Radiation Exposure (<50 mGy)**
**Case:**
A 28-year-old woman had CT KUB (18 mGy) before realizing she was 4 weeks pregnant.
* Reassure — no increased risk
* Routine antenatal care
* No need for special monitoring
---
# **3. Warfarin Embryopathy**
**Case:**
Baby born with **nasal hypoplasia, stippled epiphyses**, short limbs. Mother took warfarin at 7–10 weeks.
**Diagnosis:** Warfarin embryopathy.
**Management:**
* Switch mother to LMWH
* Cardiac + neurodevelopmental evaluation of infant
* Orthopedic follow-up
---
# **4. SLE Anti-Ro → Congenital Heart Block**
**Case:**
Mother with SLE (anti-Ro +). At 28 weeks, fetus has HR 55 bpm.
**Diagnosis:** Fetal complete heart block.
**Management:**
* Weekly fetal echocardiography
* Consider maternal dexamethasone to reduce inflammation
* Delivery planning at tertiary center
* Pacemaker may be needed postnatally
---
# **5. Maternal Phenylketonuria (PKU)**
**Case:**
Mother not compliant with low-phenylalanine diet → baby has **microcephaly + congenital heart disease**.
**Diagnosis:** Maternal PKU embryopathy.
**Management:**
* Strict low-phenylalanine diet preconception + throughout pregnancy
* Serial fetal growth scans
* Screen newborn for CHD, developmental delay
---
# **6. Isotretinoin Exposure**
**Case:**
Mother used isotretinoin for acne → baby with **microtia, conotruncal defects, thymic hypoplasia**.
**Diagnosis:** Retinoic acid embryopathy.
**Management:**
* Detailed cardiac imaging
* ENT evaluation
* Immune system assessment
* Counseling: avoid pregnancy for 1 month after stopping isotretinoin
---
# **7. Hyperthermia → Neural Tube Defect Risk**
**Case:**
Mother had continuous fever (39.5°C) at 4 weeks and used sauna.
**Diagnosis:** Risk of NTD due to hyperthermia.
**Management:**
* High-dose folic acid
* Level-II anomaly scan at 18–20 weeks
* Counsel to avoid saunas/hot tubs
---
# **8. CMV Infection**
**Case:**
Baby has **periventricular calcifications, microcephaly, deafness**.
**Diagnosis:** Congenital CMV.
**Management:**
* PCR of saliva/urine
* Antiviral therapy (valganciclovir) for newborn
* Hearing, neurodevelopmental follow-up
* Counseling about dose–response effects
* Explain “all-or-none” phenomenon at pre-implantation stage
* Optimize radiation safety protocols
---
# ✅ WANT THESE IN HTML EXAM MODE?
I can convert all **25 case scenarios** into:
✔ interactive exam-mode HTML
✔ collapsible answers
✔ JSON file for your website
✔ Printable PDF
✔ Add 25 or 50 more cases
Just tell me **which format you want next.**
Here is your **complete, high-yield, concise-but-exhaustive medical note on CMV (Cytomegalovirus)** — written in your preferred **NEET PG / INICET master-note pattern**.
* No vaccine available.
* Pregnant women → avoid sharing utensils, food, kissing toddlers on mouth, frequent handwashing.
* Universal screening **not** recommended currently.
* Blood products: **leukoreduced, CMV-negative** for neonates/immunocompromised.
---
# **10. High-Yield Exam Points**
* **MC congenital infection worldwide → CMV**
* **Periventricular calcifications = CMV**
* Rubella → **subepicardial calcifications**
* Primary maternal infection = **highest fetal risk**
* **Hearing loss = most common sequela**
* Amniocentesis after **21 weeks**, ≥6 weeks after infection for accurate PCR
* Valganciclovir → **only for symptomatic neonates**
---
If you want, I can also provide:
✅ **20 MCQs (NEET PG + INICET level)**
✅ **HTML + CSS + JS exam-mode interface**
✅ **SEO title, description, keywords**
Just tell me **“cmBelow is your **complete, concise but exhaustive medical reference note on *Toxoplasma gondii* infection*** — structured exactly in the pattern you prefer (definition → pathophysiology → causes → clinical features → investigations → differential diagnoses → management → full drug details → pregnancy considerations → prevention).
Toxoplasmosis is an infection caused by **Toxoplasma gondii**, an obligate intracellular protozoan parasite.
Transmission occurs by **ingestion of oocysts**, **tissue cysts in meat**, **transplacental spread**, **blood transfusion**, or **organ transplant**.
---
## **2. Pathophysiology**
* Parasite exists in 3 forms:
* **Oocysts** (shed from cat feces; infectious after 1–5 days).
* **Tachyzoites** (rapidly dividing; cause acute infection; cross placenta).
* **Bradyzoites** (slow, encysted; cause chronic latent infection in brain, muscle).
* Primary infection in pregnancy → *parasitemia* → **placental invasion → fetal infection**.
* Immunocompromised individuals cannot contain tachyzoites → **necrotizing encephalitis**, pneumonitis, chorioretinitis.
* **Indication**: Maternal infection (prevent fetal infection)
* **Mechanism**: Macrolide (inhibits 50S ribosome)
* **Dose**: 1 g every 8 hours
* **Adverse effects**: GI upset
* **Note**: Not effective for established fetal infection
---
### **TMP-SMX**
* Used for prophylaxis in HIV
* Dose: 1 DS daily
* Contraindications: sulfa allergy
---
## **9. Prevention**
* Avoid cleaning cat litter boxes
* Wash hands after handling soil
* Wash vegetables thoroughly
* Avoid undercooked meat
* Pregnant women should avoid raw/undercooked meat
* HIV patients: TMP-SMX prophylaxis when **CD4 <100**
---
## **10. High-Yield Exam Pearls**
* **Congenital triad**: hydrocephalus + chorioretinitis + diffuse intracranial calcification
* **IgG avidity** is the best tool for timing infection
* For non-infected fetus → **spiramycin**
* For infected fetus → **pyrimethamine + sulfadiazine + folinic acid**
* HIV with multiple ring-enhancing lesions: treat presumptively for toxoplasmosis first
---
If you want, I can also generate:
✅ 20 NEET PG + INICET MCQs
✅ A stylish HTML+CSS+JS MCQ exam page
✅ SEO title, meta description & keywords
✅ Complete “Toxoplasmosis in Pregnancy” note
✅ Image/diagram generation
Just tell me.
v mcq set”** or **“make in exam mode”**.
Parvovirus B19 – Complete Clinical Master Note
1. Definition
Parvovirus B19 is a single-stranded DNA virus (Parvoviridae family) that infects erythroid precursor cells in bone marrow via the P antigen, causing a spectrum of diseases: erythema infectiosum (fifth disease), transient aplastic crisis, hydrops fetalis, and arthropathy.
2. Virology & Pathophysiology
Smallest DNA virus; non-enveloped, ssDNA.
Targets erythroid progenitors in bone marrow → pure red cell aplasia.
Infection leads to:
Viremia (high viral load) → early flu-like symptoms.
Rubella (German measles) is a **mild viral exanthem illness** caused by **Rubella virus (Togaviridae; ssRNA)**.
Most significant for **teratogenicity** → causes **Congenital Rubella Syndrome (CRS)** if maternal infection occurs in early pregnancy.
---
## **2. Epidemiology**
* Common in **children**; outbreaks where vaccination coverage is poor.
* Humans are only known reservoir.
* Transmission: **respiratory droplets**, congenital infection.
* **1st dose: 9–12 months (India)**
* **2nd dose: 15–18 months** or at school entry
* **Contraindicated in pregnancy & severe immunosuppression**
* Women should avoid pregnancy for **1 month** after vaccination.
### **Post-exposure prophylaxis**
* **No role for immunoglobulin** to prevent CRS (only reduces maternal symptoms)
* Pregnant unvaccinated women: counselling + monitor IgG/IgM titers
---
## **10. Drug Therapy Details (for symptom relief)**
(Rubella requires only symptomatic treatment; drugs below are supportive.)
If you want, I can generate:
✅ **20 case-based MCQs (NEET PG + INI-CET level)**
✅ **HTML + CSS + JS exam mode** (stylish, like your Streamora/LWT MCQ grids)
✅ **SEO title + excerpt + long-tail keywords**
Just tell me **“MCQs”** or **“Give exam mode HTML”**.
Below is your **complete, high-yield, exam-ready Varicella Zoster Virus (VZV)** medical note — concise but exhaustive exactly as you prefer (NEET-PG + INICET gold standard).
Herpes zoster reactivation → inflammation of sensory nerves → **dermatomal pain + vesicles**.
Post-herpetic neuralgia due to neuronal damage and persistent nociceptor hyperactivity.
---
## **3. Epidemiology**
* Chickenpox: common in children.
* Zoster: increases with age (>50 yrs), immunosuppressed, HIV, malignancy, transplant.
---
## **4. Risk Factors**
### **For Primary Infection (Varicella)**
* Non-immune individuals
* Unvaccinated children
* Exposure in household/community outbreaks
### **For Reactivation (Zoster)**
* Age >50
* Immunosuppression (HIV, steroids, cancer, transplant)
* Stress
* Trauma over dermatome
---
## **5. Clinical Features**
### **A. Varicella (Chickenpox)**
* **Prodrome:** fever, malaise, sore throat
* **Rash:** “**dew drop on a rose petal**”
* Vesicles, pustules, crusts **in different stages**
* Starts on face & trunk → spreads centrifugally
* **Pruritus is prominent**
* Contagious **48 hours before rash** until **all lesions crust**.
* **Severe dermatomal pain** → vesicles along a single dermatome
* Thoracic > trigeminal involvement
* Does **not cross midline**
* May have fever, malaise.
* **Adults:** 800 mg PO **5× daily for 5 days**
* **Immunocompromised:** IV acyclovir 10 mg/kg every 8 hours
---
### **B. Herpes Zoster (Shingles)**
Start antivirals **within 72 hours** of rash onset.
**Acyclovir:** 800 mg PO 5× daily × 7 days
**Valacyclovir:** 1 g PO TID × 7 days (preferred, better absorption)
**Famciclovir:** 500 mg PO TID × 7 days
* Pregnant women
* Immunocompromised
* Newborns of mothers with varicella 5 days before to 2 days after delivery
---
## **10. Drug Summary (Exam-Focused)**
### **Acyclovir**
* **MOA:** Inhibits viral DNA polymerase after phosphorylation by viral thymidine kinase
* **PK:** Renal excretion
* **Side effects:** Crystalluria, nephrotoxicity, neurotoxicity
* **Interactions:** Avoid nephrotoxic drugs
* **Monitoring:** Renal function
* **Counselling:** Hydrate well, complete full course
### **Valacyclovir**
* Prodrug of acyclovir — better oral absorption
* Same precautions
### **Famciclovir**
* Prodrug → penciclovir
* Used for zoster
---
## **11. Pregnancy Considerations**
* Varicella in 1st–2nd trimester → **Congenital varicella syndrome** (limb hypoplasia, cataracts, microcephaly, skin scarring)
* Peripartum infection: neonatal varicella
* Live vaccine **contraindicated in pregnancy**
* Use **VZIG** for exposure
---
## **12. High-Yield Exam Lines**
* “Dew drop on a rose petal” → VZV
* Multiple stages of rash present together → Varicella
* Pain precedes rash → **Herpes zoster**
* Ophthalmic branch of CN V involvement → emergency
* PHN more common >60 years
* Tzanck smear → multinucleated giant cells
* Acyclovir needs viral thymidine kinase for activation
---
If you want, I can also generate:
✅ **Case-based 25 MCQs in HTML + CSS + JS exam mode**
✅ **Diagram/image generation of varicella vs zoster**
✅ **SEO-rich article for your website**
Just tell me!
Below is your **complete, concise-but-exhaustive medical reference on ZIKA VIRUS** — written in the same *premium clinical + exam-ready style* you prefer.
Zika virus is an **arthropod-borne Flavivirus** transmitted mainly by *Aedes aegypti* and *Aedes albopictus*.
Known for **congenital Zika syndrome (CZS)** causing microcephaly and severe fetal anomalies.
* Long sleeves
* DEET repellents
* Avoid travel to Zika-endemic areas in pregnancy
### **C. Sexual Transmission Prevention**
* Condom use for **≥3 months** after male infection
* **≥2 months** after female infection
---
## **10. Key Exam Points**
* Zika = **maculopapular rash + conjunctivitis + mild fever**
* Severe fetal microcephaly = **Congenital Zika Syndrome**
* Best diagnostic test = **RT-PCR**
* No NSAIDs until dengue ruled out
* Highest fetal damage in **1st trimester**
* Vector = **Aedes** (day-biting)
---
If you want, I can also generate:
✅ **25 NEET PG / INICET-style MCQs**
✅ **HTML + CSS + JS exam-mode MCQ module**
✅ **SEO-rich article version** for your medical hubs
✅ **Infographic-style generated image**
Just tell me **“give MCQs”** or **“give SEO article”** or **“generate image”**.